The authors are with Quality Milk Production Services, Cornell University.
Many research investigators have clearly shown the cow’s immune system is doing a good job for the majority of cases where there is no detectable organism (“no growth” on most culture media) or E. coli. This work has been repeatedly and convincingly done by mastitis workers across the U.S. in the Northeast at Cornell, the Upper Midwest at the University of Wisconsin-Madison and Michigan State, the West in California, and even in New Zealand.
The list leader
“No growth” is the most common result associated with clinical mastitis. If samples are taken hygienically and cultured appropriately, it is very typical for 25% to 35% of the results to not have a culturable organism at the time mastitis is detected. Most often, this indicates the cow’s immune system has dealt with the pathogen and what is seen as abnormal milk (clots, flakes, and so forth) is the normal inflammatory results.
If there is not an active, major pathogen to be killed with an antibiotic, there is likely little reason to spend the time, money, hospital pen space, and milk discard that comes from administering antibiotic tubes. The biological research done in those on-farm trials mentioned earlier shows there is little to no difference in milk production, recurrence of clinical mastitis, future somatic cell count (SCC), or culling between those cows administered Food and Drug Administration (FDA) approved antibiotics and those not treated after a no-growth culture result.
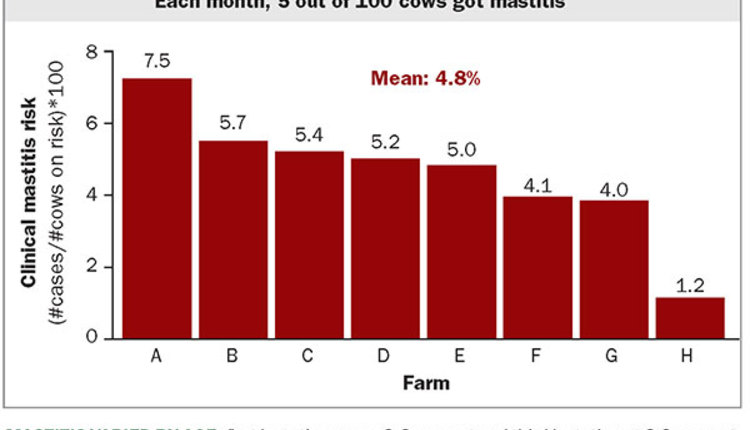
Recently, we have looked closely at the milk loss associated with various diagnostic outcomes after clinical mastitis, including no growth. For one year, Quality Milk Production Services received a milk sample from every clinical mastitis case among about 15,000 cows on eight commercial dairy farms. We used National Mastitis Council (NMC) culture methods followed by MALDI-ToF technology to identify pathogens associated with these cases. Of the 7,515 cases, 30% resulted in no detectable pathogen or no growth. This situation was fairly consistent among farms.
Less milk lost
When there is no growth, the total milk loss was not more than 90 pounds for primiparous cows and 120 pounds for multiparous compared to control cows without mastitis. For comparison, primiparous and multiparous cows with Strep. dysgalactie mastitis lost approximately 520 and 450 pounds of milk, respectively, and the effects lasted longer.
If these cows with no growth mastitis were treated with a typical antibiotic protocol (three days of tubes administered once a day and 72 hours milk withhold after treatment), that would result in at least six days of milk discard.
For roughly 100 pounds of milk loss, depending a bit on parity and an optimistic milk price of $20 per cwt., that is a $20 loss in milk from a no-growth case. This calculation is based on a cow that is left untreated and in the hospital pen for three days while the milk is abnormal, on average. If we observe the Pasteurized Milk Ordinance (PMO), this is a sunk cost because we are not to sell abnormal milk for human consumption.
We observed that three days after the onset of clinical mastitis where no mastitis pathogen was detected, the first-lactation cows were making, on average, 45 pounds per day and second- and greater-lactation cows were back to making 70 pounds per day. If that normal milk was discarded during 72 hours of milk withholding at $20 per cwt., it would be $27 and $42 of dumped milk that could be sold per case.
So, paying $12 for three days of mastitis treatment cost, plus $27 or $42 in additional discarded milk, the cost of treating no-growth cases would be approximately two times or three times higher, depending on parity and including the cost of mastitis diagnostics, than not treating and holding the cow out of the tank while the milk is abnormal. This shows you would lose money by treating clinical mastitis cases where there was no growth.
Better observation
However, it is important to not sell milk unfit for human consumption as outlined by the PMO. In the development of a recent series of online training modules as part of a northern New York agriculture development grant, we spent some time exploring how farms decide when to put a cow’s milk back into the saleable milk tank after a mastitis event.
Based on the 15 farms on this project, there was quite a bit of variation in how this was performed and how well the farm personnel were trained in this area. Most farms were stripping cows and visually observing the milk on the deck, although one farm was using a strip cup and one farm was performing a California Mastitis Test (CMT).
Added a tool
For the training module, which is available at dairyroutines.com, we provided strip cups with a sieve on the top to the farms. The protocol in the module is to first check the milk withhold time if the cow has been treated with antibiotics to make sure the cow is beyond the withhold time. Discard three strips of milk if you are checking the cow premilking, and then, either pre- or postmilking, squirt seven to 10 strips of milk on to the sieve of the strip cup. Visually observe the sieve of the strip cup, and if there are no clots, flakes, or blood, the milk can go back into the saleable milk tank.
The feedback from the farms after starting the new protocol is that using the strip cup has helped make the process simpler and easier to train new employees on. We would encourage you to evaluate this process on your farm to make sure it is being performed correctly.
Overall, we can save money, prudently use antibiotics, reduce hospital pen density, and continue to produce nutritious food for human consumption by not treating clinical mastitis cases where no mastitis pathogen is detected by conventional techniques. Coupling this with a good protocol for when to return a cow’s milk to the tank after a mastitis case can ensure that you continue to ship high-quality milk from your dairy.